Dr Surangi Mendis, an audiovestibular consultant at UCLH, explains more about this challenging condition
Vestibular migraine (VM) and Ménière’s disease (MD) are distinct but overlapping disorders. Up to 51% of MD patients may have VM-MDOS [1], whilst a smaller proportion of VM patients may also meet VM-MDOS criteria [2]. This blog piece outlines the presentation, diagnosis and management of VM-MDOS, offering guidance for headache specialists.
Some Background on this topic
Vestibular Migraine is a neurological diagnosis characterised by recurrent vertigo, dizziness, or unsteadiness with migraine features, with a lifetime prevalence of 1-3% [3]. Ménière’s disease, in contrast, is an inner ear disorder marked by episodic vertigo, hearing loss, tinnitus, and/or aural fullness. MD can be linked to endolymphatic hydrops (accumulation of endolymphatic fluid within the inner ear), detectable via imaging.
Endolymphatic hydrops can occur in two forms:
- Idiopathic endolymphatic hydrops = MD.
- Secondary hydrops: Resulting from trauma, autoimmune disease, or local pathology.
Diagnosis: Identification of VM-MDOS can be challenging. Patients must meet diagnostic criteria for both VM and MD:
- ICHD-3 criteria for VM [4]:
- ≥ 5 vestibular episodes (5 minutes-72 hours).
- Current or past migraine history.
- Migraine features in ≥50% of vestibular episodes (e.g., unilateral headache, photophobia, or aura).
- Exclusion of other diagnoses.
- Consensus criteria for Ménière’s disease [5, 6]:
- ≥ 2 spontaneous vertigo episodes (20 minutes-12 hours).
- Audiometrically documented low- to medium-frequency sensorineural hearing loss.
- Fluctuating aural symptoms (hearing, tinnitus, fullness).
- Exclusion of other vestibular diagnoses.
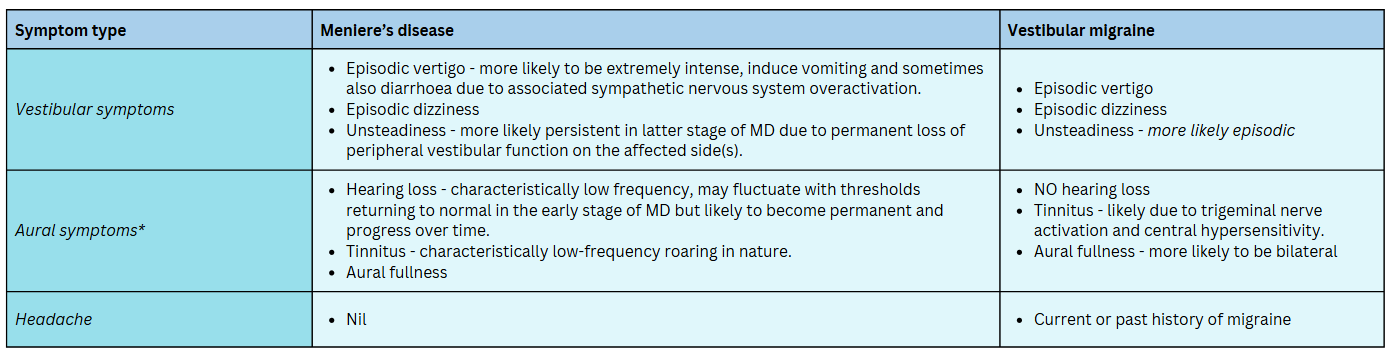
Signs and symptoms: A summary and comparison of the presenting symptoms in MD and VM is given in Table 1:
Pathophysiology
VM is thought to result from activation of the trigeminovascular system, causing neurogenic inflammation, chemical signalling changes, and cortical spreading depression in vestibular pathways [7 - 9].
MD stems from abnormal endolymphatic fluid accumulation, disrupting local cochlear and vestibular function. Shared triggers (stress, diet) and mechanisms may contribute to development of VM-MDOS, though the exact pathophysiology remains unclear.
Investigations
Clinical assessment and targeted investigations are undertaken:
- History: Characterise vertigo episodes, aural symptoms, and migraine associations.
- Examination: Eye movements are particularly useful. During a Meniere’s episode, there are distinct phases: irritative, paralytic, and recovery, each with specific patterns of nystagmus [10, 11].
- Audiometry: Documentation of fluctuating, low-frequency hearing loss characteristic of MD.
- Vestibular tests: Vestibular tests, e.g. caloric, may identify loss of vestibular function on the affected side(s) in MD [6].
- Imaging (*NEW*): Delayed gadolinium-enhanced MRI (FLAIR) visualises endolymphatic hydrops, helping to distinguish MD from VM [12 - 14].
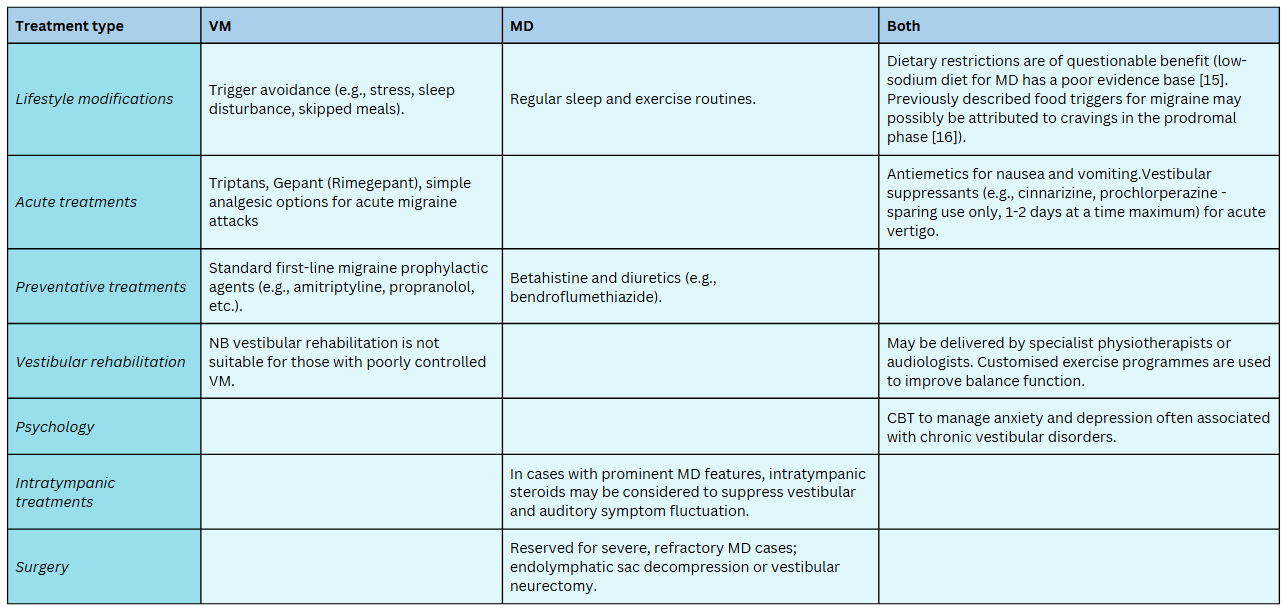
Management: Treatment of both VM and MD should occur in tandem. A multidisciplinary approach is ideal. Treatment strategies are outlined in table 2:
Long-term management and prognosis: The prognosis of VM-MDOS varies widely. Those with active VM-MDOS should remain under ENT or audiovestibular review (in addition to headache follow up) to:
- Monitor hearing loss and provide rehabilitation (e.g., hearing aids, tinnitus counselling).
- Adjust treatments based on symptom changes.
- Address occupational restrictions, e.g. MD-associated vertigo prohibits operating machinery or working at heights.
Driving restrictions typically apply, as VM-MDOS patients often experience spontaneous disabling vertigo. DVLA guidance is as follows: ‘You must tell DVLA if you experience dizziness that is sudden, disabling or recurrent’. Further information: Dizziness or vertigo and driving - GOV.UK [17].
Conclusion
VM-MDOS is a complex overlap syndrome requiring individualised care. Future research should clarify its mechanisms, define diagnostic criteria, and evaluate treatments, including newer anti-CGRP migraine therapies.
Key message for headache clinicians: VM-MDOS should be considered in VM patients with fluctuating hearing loss (note this refers specifically to hearing loss, rather than aural fullness – the latter can overlap with both VM and MD). Please refer for ENT or audiovestibular evaluation.

Dr Surangi Mendis
Consultant in Audiovestibular Medicine
University College London Hospitals NHS Foundation Trust
References:
- Ghavami Y, Mahboubi H, Yau AY, Maducdoc M, Djalilian HR. Migraine features in patients with Meniere's disease. Laryngoscope. 2016;126(1):163-168. doi:10.1002/lary.25344
- Shin CH, Kim Y, Yoo MH, et al. Management of Ménière's Disease: How Does the Coexistence of Vestibular Migraine Affect Outcomes?. Otol Neurotol. 2019;40(5):666-673. doi:10.1097/MAO.0000000000002176
- Baloh RW. Vestibular Migraine I: Mechanisms, Diagnosis, and Clinical Features. Semin Neurol. 2020;40(1):76-82. doi:10.1055/s-0039-3402735
- ICHD-3 criteria for vestibular migraine. Available at: https://ichd-3.org/appendix/a1-migraine/a1-6-episodic-syndromes-that-may-be-associated-with-migraine/a1-6-6-vestibular-migraine/
- Lopez-Escamez JA, Carey J, Chung WH, et al. Diagnostic criteria for Menière's disease. J Vestib Res. 2015;25(1):1-7. doi:10.3233/VES-150549
- Basura GJ, Adams ME, Monfared A, et al. Clinical Practice Guideline: Ménière's Disease. Otolaryngol Head Neck Surg. 2020;162(2_suppl):S1-S55. doi:10.1177/0194599820909438
- Espinosa-Sanchez JM, Lopez-Escamez JA. New Insights Into Pathophysiology of Vestibular Migraine. Frontiers in Neurology. 2015;6:12. doi:10.3389/fneur.2015.00012. PMID: 25705201.
- Furman JM, Marcus DA, Balaban CD. Vestibular Migraine: Clinical Aspects and Pathophysiology. The Lancet. Neurology. 2013;12(7):706-15. doi:10.1016/S1474-4422(13)70107-8. PMID: 23769597.
- Russo A, Marcelli V, Esposito F, et al. Abnormal Thalamic Function in Patients With Vestibular Migraine. Neurology. 2014;82(23):2120-6. doi:10.1212/WNL.0000000000000496. PMID: 24814847.
- Lee SU, Kee HJ, Sheen SS, Choi BY, Koo JW, Kim JS. Head-shaking and Vibration-induced Nystagmus During and Between the Attacks of Unilateral Ménière's Disease. Otol Neurotol. 2015;36(5):865-872. doi:10.1097/MAO.0000000000000743
- Fukushima M, Waki S, Makino S, Akahani S. Factors associated with spontaneous nystagmus changes in acute Ménière's disease. J Neurol. 2024;271(10):6588-6595. doi:10.1007/s00415-022-11367-6
- Li J, Li L, Jin X, et al. MRI can help differentiate Ménière's disease from other menieriform diseases. Sci Rep. 2023;13(1):21527. Published 2023 Dec 6. doi:10.1038/s41598-023-49066-5
- Imai T, Uno A, Kitahara T, et al. Evaluation of endolymphatic hydrops using 3-T MRI after intravenous gadolinium injection. Eur Arch Otorhinolaryngol. 2017;274(12):4103-4111. doi:10.1007/s00405-017-4739-9
- Pai I, Mendis S, Murdin L, Touska P, Connor S. Magnetic resonance imaging of Ménière's disease: early clinical experience in a UK centre. J Laryngol Otol. 2020;134(4):302-310. doi:10.1017/S0022215120000626
- Webster KE, George B, Lee A, et al. Lifestyle and dietary interventions for Ménière's disease. Cochrane Database Syst Rev. 2023;2(2):CD015244. Published 2023 Feb 27. doi:10.1002/14651858.CD015244.pub2
- Karsan N, Bose P, Newman J, Goadsby PJ. Are some patient-perceived migraine triggers simply early manifestations of the attack?. J Neurol. 2021;268(5):1885-1893. doi:10.1007/s00415-020-10344-1
DVLA Dizziness or Vertigo and Driving. Available at: Dizziness or vertigo and driving - GOV.UK
Dr Surangi Mendis is also GP-trained and is a member of our GPwER group. If you are a GP interested in Headache, find out more about this active group here.